
Inflammatory Bowel Disease and Disordered Eating

Inflammatory Bowel Disease and Disordered Eating from a Nutrition Perspective
Individuals with IBD have a complex relationship with food, and it’s one that hasn’t been highlighted enough in scientific and psychological literature. Thankfully, interest and awareness are growing, which typically means the research will follow!
This area is crucial to discuss, especially working with IBD patients who might also be on dietary therapy.
At present, we do not have a specific screening tool for disordered eating behaviors in the pediatric IBD population. Years of working with this population have taught me that the relationship between IBD and nutrition is intricate and that disordered eating patterns are common.
One needs to be mindful and aware of each individual’s needs. Health professionals should meet IBD patients where they are, then work with them to customize a plan for altering their nutrition or implementing diet therapy.
The purpose of this in-depth article is to provide current information and recommendations surrounding disordered eating from a nutrition perspective for those with IBD or if you are caring for someone with IBD.
Disclaimer: This article is intended for informative purposes and is not intended for medical or mental health counsel. Some elements may be triggering.

Photo by Andres Ayrton from Pexels
What Is the Link Between IBD and Disordered Eating?
Research has demonstrated higher rates of mental disorders, including depression and anxiety, in patients with IBD compared to patients without IBD (1, 2). However, other psychosomatic impacts of IBD on an individual’s well-being have received minimal attention in the literature.
An exceptionally important topic (that is gaining attention among providers and patients) is the increased prevalence of disordered eating patterns in the IBD population. Research suggests a high risk for the development of disordered eating patterns and negative body image in patients with diet-related chronic illnesses (including celiac disease, type I diabetes, and IBD) and the limited IBD-specific literature so far supports this as well (3).
Patients with IBD are at risk of:
- Impaired digestion, absorption, and metabolism
- Nutrient deficiencies
- Body shape and weight fluctuations related to disease and therapy treatments
- Decreased appetite or alteration of hunger cues
I will add that most patients don’t know about these predispositions when they are diagnosed. They are not given proper warning that they may or may not face many of these challenges.
Up to 40% of IBD patients have attempted various diet therapies – often without the assistance of a physician or dietitian (4). The truth is that food avoidance can increase the risk for malnutrition and may have mixed effects on IBD symptoms.
This is especially vital among pediatric patients, who are more vulnerable to negative outcomes caused by disordered eating patterns. They need to maintain adequate growth and meet developmental milestones, such as puberty. This is difficult if the patient isn’t receiving adequate nutrition and calories.
IBD and disordered eating patterns are a rarely discussed topic at gastrointestinal (GI) appointments due to numerous factors, such as:
- Time and number of patients to see
- Medical therapy treatment is priority
- Lack of awareness around this topic
- Lack of access to a multidisciplinary team with experts in this area
- New complexity of dietary therapy frequently without appropriate oversight

Disordered Eating vs. Eating Disorder
Before diving into the research on the association between IBD and disordered eating, let’s first differentiate between disordered eating and an eating disorder.
Let’s break it down (5, 6):
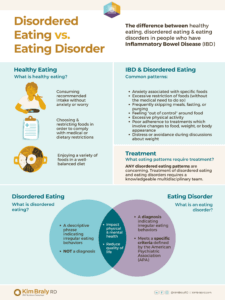
Healthy Eating
- Consumes recommended calories and foods without anxiety or worry about intake
- Chooses and/or restricts foods as medically implicated in order to comply with prescribed dietary restrictions
- Enjoys consuming a variety of foods within a well-balanced diet
Disordered Eating
- Is a descriptive phrase indicating irregular eating behaviors, not a diagnosis
- Involves unhealthy thoughts and behavior which impact medical and mental health
- Negatively impacts an individual’s quality of life
Eating Disorder
- Is a diagnosis indicating irregular eating behaviors meet specific criteria defined by American Psychiatric Association (APA)
- Involves unhealthy thoughts and behaviors which impact medical and mental health
- Negatively impacts an individual’s quality of life
The most significant difference between disordered eating and an eating disorder is whether or not the individual’s symptoms and experiences meet the criteria defined by the APA. Both share similar thought patterns and behaviors related to food, weight, and/or body shape, which negatively impact the individual’s quality of life.

Disordered eating patterns in IBD patients can present in many different ways and may include (5, 6):
- Anxiety associated with specific foods
- Excessive restriction of foods when not medically indicated
- Frequent meal skipping, fasting, or purging
- Feeling a loss of control around food
- Excessive physical activity
- Significant concerns or poor adherence to treatments which involve changes to foods, weight, or body appearance
- Poor adherence to treatments in order to alter weight or body appearance
- Distress or avoidance when discussing weight
The specific and narrow criteria for diagnosis of an eating disorder may exclude a majority of patients suffering from disordered eating patterns. It is important that providers and patients alike understand that ANY disordered eating patterns are concerning, deserving both attention and treatment, as they can progress into nutrition deficiencies or other serious illnesses.
Additionally, disordered eating patterns can impact physical and mental health in other ways such as bone loss, gastrointestinal disturbances, electrolyte and fluid imbalances, low heart rate and blood pressure, increased anxiety, depression, and social isolation (6).

Complex Relationship Between IBD and Eating Patterns
Current literature exploring disordered eating patterns in patients with IBD is limited to case studies describing clinicians’ individual experiences with patients, observational studies, and some cross-sectional studies.
Overall, the current evidence suggests that IBD is positively associated with body image concerns and disordered eating patterns.
Below we highlight two of the most recent studies:

Disordered Eating, Body Dissatisfaction, and Psychological Distress (2)
Publish Date: March 14, 2020
Study Design: Anonymous cross-sectional survey study, data collected from single outpatient adult IBD center
Aim: Prevalence of disordered eating patterns in patients with IBD and factors associated with disordered eating using the EAT-26
Results:
- 81% responded affirmatively to at least 1 of 7 items which researchers deemed to represent disordered eating patterns
- 13% met screening cutoff where further evaluation for an eating disorder is recommended
- Elevated EAT-26 scores associated with: Females, underweight, IBD diagnosed during childhood, psychological distress, and body image disturbances
Assessing the Prevalence of and Risk Factors for Disordered Eating Attitudes and Behaviors in Adolescents with IBD (7)
Publish Date: June 9, 2021
Study Design: Multisite cross-sectional study, data collected from sites in the ImproveCareNow quality improvement collaborative
Aim: Prevalence of disordered eating patterns in adolescents with IBD and factors associated with disordered eating
Results:
- 30% reported body image concerns
- 10% reported disordered eating patterns
- Factors significantly associated with disordered eating behaviors: Patients with high anxiety, a greater number of years since diagnosis
Note: Cross-sectional studies can only suggest associations between variables and are unable to make causal claims. Meaning, IBD and disordered eating patterns can be associated but researchers cannot claim that IBD leads to (or causes) disordered eating patterns.

IBD-Specific Risk Factors for Disordered Eating
Risk factors have been identified which may increase the likelihood that a patient with IBD will develop disordered eating patterns (2, 7):
- Heightened focus on weight changes
- IBD symptoms related to inflammation
- Dietary restriction
- Weight and body shape fluctuations
- Recommendations from friends and family
- Lack of IBD-knowledgeable multidisciplinary team support

IBD Symptoms & Dietary Restriction
Due to the nature of IBD, symptoms ebb and flow and are influenced by medications, food, and the environment. Symptoms vary from patient to patient and include:
- Cramping
- Abdominal pain
- Indigestion
- Nausea
- Gas/bloating
- Bowel urgency
- diarrhea
- Constipation
- General fatigue and weakness
These IBD symptoms and the chronic nature of the disease can greatly impact a patient’s quality of life. Studies have shown that patients with IBD report significant declines in their quality of life and increased psychological distress including social isolation.
Many strongly believe that certain foods will trigger symptoms, so it is no surprise that patients are often interested in how diets impact their disease activity. This may drive patients to restrict certain foods/food groups or overall energy intake, either independently or with clinician guidance.
Modifying dietary patterns also allows the patient to actively participate in their IBD nutrition management at every meal and snack, which may provide the patient a sense of control over their disease activity (9). However, eliminating some foods/food groups can improve symptoms but may ultimately exacerbate a patient’s malnutrition or feeling of social isolation. Both malnutrition and social isolation are associated with a significant reduction in quality of life in patients with IBD. (1)
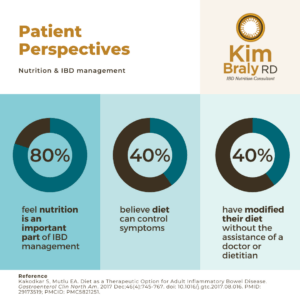
Patient Perspectives on IBD Nutrition and Management (9)
- 80% feel nutrition is an important part of IBD management
- 40% believe diet can control Inflammatory Bowel Disease symptoms
- 40% have modified diet without assistance of MD/RD – food avoidance can increase risk for malnutrition
Additionally, implicit in dietary therapy is an overall increased dietary awareness which requires hyperfocus on ingredient lists and developing a sense of morality around food choices (“legal” vs “illegal” foods). Studies suggest that any type of restrictive diet may contribute to a patient’s risk for disordered eating patterns (2). This highlights the importance of multidisciplinary team support surrounding nutrition for these patients.
Patients may also receive dietary recommendations from different practitioners, support groups, blogs, and friends, which can be overwhelming and, in some cases, contradictory. This type of input may also contribute to disordered eating patterns.
Dietary therapy is generally safe, effective, and well-tolerated, and is increasingly prescribed in the management of IBD nutrition and symptoms. However, it’s important to be aware that it can affect disordered eating patterns in this population. This is why it’s crucial that dietary therapy for IBD management happen under the care of a collaborative, multidisciplinary team.

Weight and Body Shape Fluctuations
Fluctuations in weight and body shape are common IBD side effects due to disease state activity, medications, dietary therapies, and surgical management. It’s common for patients to lose weight during a flare and gain weight once in remission as their nutrition status improves (2).
Medically, corticosteroids are frequently used during a flare-up which may cause weight gain and a change in body composition. In other instances, a surgical procedure may be required which can change body shape and appearance (1).
Lastly, a prescribed dietary therapy can lead to rapid weight fluctuations. The care of an experienced dietitian and mental health provider can help positively impact patient perception and expectation of weight fluctuations from flares to recovery and remission periods.
Patients with IBD often express body image dissatisfaction, which the literature suggests is a key risk factor for the development of disordered eating patterns. These concerns over body image include both undesirable weight loss or inability to gain weight, with concerns around appearing “ill” or “too thin.”
Patients express concern with weight gain during periods of remission as they improve their nutrition status. These concerns may be exacerbated by the medical attention to a patient’s weight compounded by societal ideals of the “perfect body,” which may heavily influence adolescents. (7).

The Importance of Multidisciplinary Team Support for Patients with IBD
My own experience and recent studies suggest the support of a collaborative, multidisciplinary team may be the key to providing the best care to patients with chronic GI conditions. This is not the traditional standard of care, as many patients are under the care of only a gastroenterologist (GI).
The studies on this traditional type of care suggest that it fails to improve quality of life, and patient dissatisfaction rates are high. GI-only care is limited in providing a more holistic approach to care due to a limited amount of time with patients, a focus on pharmacological management, and inadequate training and/or lack of resources to provide specific dietary, psychological, and other management strategies (8).Collaborative management is defined as “care that strengthens and supports self-care while assuring that effective medical, preventive, and health maintenance interventions take place” (information on who makes up this multidisciplinary team will be covered in the next section).
Collaborative Management as a Key to Patient Care
The limited research on this type of model for IBD management suggests it is associated with improved clinical outcomes compared to traditional care, including:
- Improved quality of life
- Better psychological health
- Cost-effectiveness
Cost-effective care entails critical decision-making and the best use of money and resources for an individual and their specific disease state.
The most benefit is found when there is open communication between the members of the multidisciplinary team, which may enable the team to share the identification of, and decision-making about, important clinical issues (8). The multidisciplinary team involves the patient and their family (or other network/support system) at the center.
Potential Barriers & Solutions in Collaborative Care
This model of management has been adopted by an increasing number of GI practices to best support their patients. There are barriers to providing collaborative care including lack of access to mental health providers and registered dietitians trained in IBD nutrition management, and lack of reimbursement for their services.
However, with increased access to telehealth and virtual visits, some of these barriers may be removed. With more research on the benefits of collaborative care, it is essential for GI practices to identify barriers and move in the direction of multidisciplinary team management. We are hopeful that research regarding the multidisciplinary team approach will continue to grow.
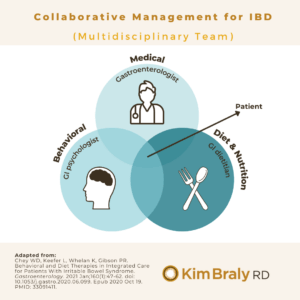
The Ideal Multidisciplinary Team for IBD Care
To properly care for patients with IBD and disordered eating struggles, the multidisciplinary team should share common goals. These should include goals for disease management, improving overall symptoms, and enhancing the patient’s well-being and quality of life.
The team must value the importance of medications, dietary modifications, and behavioral interventions to provide the greatest likelihood of success for patients with IBD. This type of management can be summed up with the phrase “a whole is greater than the sum of its parts”(8). Ideally, the team provides a united front and messaging.
What providers make up this collaborative, multidisciplinary team?
An ideal multidisciplinary team includes:
(1) Gastroenterologist/GI provider
- Presents IBD treatment options and oversees treatment management to control disease
- Expert in medication management including but not limited to side effects, lab monitoring, adjustments
- Refers to a multidisciplinary team for support around diet and mental health, insurance challenges, etc.
(2) Mental Health Provider
- Knowledgeable in psychosomatic impacts of GI chronic disease
- Teaches cognitive behavioral therapy techniques (such as relaxation and coping strategies for anxiety)
- This could be a Psychiatrist, Psychologist, mental health NP or Clinical Social Worker with expertise in IBD/GI conditions or chronic illness
(3) Registered Dietitian
- Trained in evidence-based nutrition therapies for IBD
- Assesses nutrition intake and helps to prevent/correct nutrient deficiencies
- Identifies trigger foods and presents predisposition to eating patterns in IBD to patient
- Supports patient in food exposure and reintroduction in order to expand diet as tolerated
To learn more, check out my 3D approach to supporting a patient with IBD.

Recommendations from an IBD Dietitian
Individuals with IBD frequently experience a negative response to food. This makes sense – the gut and brain are connected. In fact, our gut is frequently referred to as the “second brain.”
If food equals pain in the presence of inflammation, one perceives an associated response to avoid that specific food. This is natural protection the body and mind can develop to adapt to a difficult situation.
While the research highlights associations between common trigger foods, each patient is unique in what they personally may identify as a “trigger” food. It’s challenging but imperative to overcome and retrain thinking around these thought patterns, encouraging intuitive eating.
Here are some strong recommendations for IBD and disordered eating screening, prevention and management
Medical, mental health or nutrition providers:
- Inform patients at diagnosis about the predisposition to restrictive eating patterns and that they will be asked at each visit about their relationship with food
- Ask about one’s relationship with food as the standard of care at each visit
- Consider incorporating screening tools such as the EAT-26
- Explain to the patient up-front that the goal is NOT diet restriction, but expansion, as disease is treated and food triggers are identified even when on a dietary treatment regimen
- Look for signs of unnecessary restrictions
- Acknowledge that social gatherings and holidays can be challenging with IBD, especially when in a flare
- Point patients to support resources for these (see below for a few)
- Treat eating disorder ASAP with referral to appropriate mental-health professional/s
- Caution patient with social media and messages communicated on social platforms in regards to diet, diet culture, and body image
Patient Advocacy – What to mention at your appointment
- Notify your GI team if you experience any of the following:
- Anxiety, unhealthy thoughts, or behaviors associated with eating or thinking about specific foods
- Anxiety or dissatisfaction around body image and/or weight changes
- Lack of enjoyment while eating or desire to skip meals
- An eating regimen that is eliminating whole food groups
The Bottom Line on IBD and Disordered Eating
Disordered eating patterns among patients with IBD is an emerging and important topic to address. Although the current research is limited, early studies are suggesting associations between IBD and disordered eating patterns and concerns with body image (5, 7).
There are many risk factors for the development of disordered eating patterns which patients with IBD are exposed to due to the nature of the disease. Support by an integrated, multidisciplinary GI team is ideal. Clinicians should take time to assess a patient’s eating behaviors and attitudes to know how to best support the patient.
To identify and intervene in disordered eating patterns as early as possible, GI-teams can utilize screening tools (such as the EAT-26) and create a workflow of screening that includes triaging to higher levels of care if needed (7). There is more research to be done on this topic so we can best support our patients with IBD in navigating the complex relationships that develop with food, eating patterns, and body image over their lifetime.
Recommended Resources
- imPACt podcast – Podcast by adolescent members of the PAC which shares perspectives of patients with IBD within the Improve Care Now network.
- Disordered Eating Toolkit – Developed by Improve Care Now which provides patient perspective on IBD, nutrition and disordered eating.
- NTforIBD: a volunteer-led non-profit organization dedicated to improving the outcomes of patients with IBD through the use of nutrition. https://www.ntforibd.org/role-nutrition-ibd/diet-depression-anxiety/
- NEDA helpline for support: https://www.nationaleatingdisorders.org/help-support/contact-helpline
- Crohns and Colitis Foundation – resources surrounding mental health
References
- Ilzarbe L, Fàbrega M, Quintero R, Bastidas A, Pintor L, García-Campayo J, Gomollón F, Ilzarbe D. Inflammatory Bowel Disease and Eating Disorders: A systematized review of comorbidity. J Psychosom Res. 2017 Nov;102:47-53. doi: 10.1016/j.jpsychores.2017.09.006. Epub 2017 Sep 14. PMID: 28992897.
- Wabich J, Bellaguarda E, Joyce C, Keefer L, Kinsinger S. Disordered Eating, Body Dissatisfaction, and Psychological Distress in Patients with Inflammatory Bowel Disease (IBD). J Clin Psychol Med Settings. 2020 Jun;27(2):310-317. doi: 10.1007/s10880-020-09710-y. PMID: 32172438.
- Satherley R, Howard R, Higgs S. Disordered eating practices in gastrointestinal disorders. Appetite. 2015 Jan;84:240-50. doi: 10.1016/j.appet.2014.10.006. Epub 2014 Oct 13. PMID: 25312748.
- Guadagnoli L, Mutlu EA, Doerfler B, Ibrahim A, Brenner D, Taft TH. Food-related quality of life in patients with inflammatory bowel disease and irritable bowel syndrome. Qual Life Res. 2019 Aug;28(8):2195-2205. doi: 10.1007/s11136-019-02170-4. Epub 2019 Mar 21. PMID: 30900206; PMCID: PMC6625837.
- David JG, Chute D, Reed B, Saeed S, DeMatteo D, Atay O, Maddux M, Daly B. Assessing the Prevalence of and Risk Factors for Disordered Eating Attitudes and Behaviors in Adolescents With Inflammatory Bowel Disease. Inflamm Bowel Dis. 2021 Jun 9:izab154. doi: 10.1093/ibd/izab154. Epub ahead of print. PMID: 34106253.
- Improve Care Now, Disordered Eating Toolkit
- https://www.eatright.org/health/diseases-and-conditions/eating-disorders/what-is-disordered-eating
- Chey WD, Keefer L, Whelan K, Gibson PR. Behavioral and Diet Therapies in Integrated Care for Patients With Irritable Bowel Syndrome. Gastroenterology. 2021 Jan;160(1):47-62. doi: 10.1053/j.gastro.2020.06.099. Epub 2020 Oct 19. PMID: 33091411.
- Kakodkar S, Mutlu EA. Diet as a Therapeutic Option for Adult Inflammatory Bowel Disease. Gastroenterol Clin North Am. 2017 Dec;46(4):745-767. doi: 10.1016/j.gtc.2017.08.016. PMID: 29173519; PMCID: PMC5821251.
Contributing Author
Courtney Lightfoot MS, Dietetic Intern through Cleveland Clinic

Hi! I'm Kim Braly, RD, a clinical researcher and IBD Nutrition Consultant. I specialize in cutting-edge dietary therapies for inflammatory bowel disease that have been shown in multicenter trials to decrease inflammation, alleviate IBD symptoms and induce remission. I'm passionate about offering this effective new option to patients and their families with my 3D-Dietary™ Approach for IBD and helping to usher in a new era of IBD treatment through mentoring and research trial consultation. Let's see what diet can do for you.
ABOUT



FOR PATIENTS

Flares Happen!
You can't always put your life on hold when IBD rears its head, but you can make this your easiest flare yet. My proven diet and lifestyle tips support your gut, body, mind & emotions for a faster recovery and a longer remission.
FOR PARENTS

Is Your Child’s Weight Dropping Fast?
You don't have to stand helpless during an IBD flare. Feed your child foods proven to minimize triggers, calm inflammation, and repair the gut. Get them healing and growing!